OMHSAS to Hold Monthly Provider Webinars
In an effort to streamline the flow of information between the Office of Mental Health and Substance Abuse Services (OMHSAS) and providers; provider associations; and consumer, family, and advocate representatives, OMHSAS will hold monthly webinars throughout 2021.
Starting in January 2021, the webinars for providers, provider associations, and consumer, family, and advocate representatives will take place on the third Tuesday of each month from 3:00 pm – 4:00 pm. They will begin on Tuesday, January 19, 2021. A separate webinar will be held with counties and county affiliates. We ask stakeholders to join in only one monthly meeting; they should choose the meeting that will best suits their interests.
OMHSAS will use this monthly time to provide general updates and discuss issues that meeting attendees will send to OMHSAS ahead of time. Recommendations for agenda topics can be submitted via email by the close of business on the second Tuesday of each month.
OMHSAS will send out email reminders for each monthly meeting. The first reminder will be sent out two weeks in advance to remind stakeholders to send in agenda topics; it will also contain webinar registration information. Another email reminder will be sent one week in advance of each meeting; it will contain only the webinar registration information.
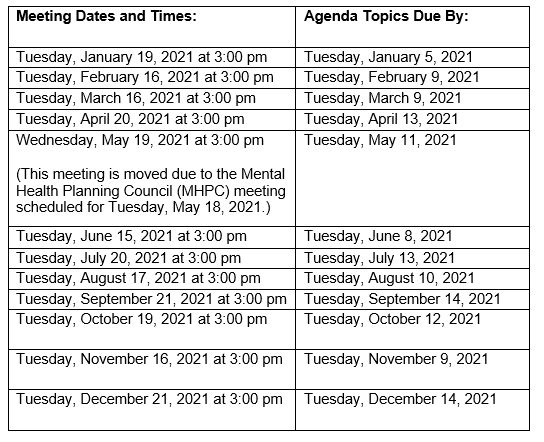
Below are the dates and times for each provider, provider association, and consumer, family, and advocate representatives meeting in 2021:
OMHSAS is open to ideas and suggestions on how they can maximize the effectiveness of these meetings with the ultimate goal of meeting the needs of OMHSAS stakeholders and staff.
If you are not currently on the OMHSAS distribution list, please contact us here.
Please register for the OMHSAS Provider/Family Member Stakeholder Meeting on January 19, 2021 at 3:00 PM (Eastern Standard Time (EST).
After registering, you will receive a confirmation email containing information about how to join the webinar.